For a client diagnosed with epistaxis, which intervention would be included in the care plan? ✅ Đầy đủ
Mẹo về For a client diagnosed with epistaxis, which intervention would be included in the care plan? 2022
Bùi Công Duy đang tìm kiếm từ khóa For a client diagnosed with epistaxis, which intervention would be included in the care plan? được Cập Nhật vào lúc : 2022-09-16 09:51:03 . Với phương châm chia sẻ Thủ Thuật về trong nội dung bài viết một cách Chi Tiết Mới Nhất. Nếu sau khi Read nội dung bài viết vẫn ko hiểu thì hoàn toàn có thể lại phản hồi ở cuối bài để Ad lý giải và hướng dẫn lại nha.Nosebleeds are common. Most often they are a nuisance and not a true medical problem. But they can be both.
Nội dung chính- Nosebleed careWhen to seek emergency careWhen to contact your doctorFrom Mayo Clinic to your inbox Nose Bleed Management and Epistaxis
Nosebleed care
- Sit upright and lean forward. By remaining upright, you reduce blood pressure in the veins of your nose. This discourages further bleeding. Sitting forward will help you avoid swallowing blood, which can irritate your stomach.Gently blow your nose. Blow your nose
to clear your nose of blood clots. Then spray both sides of your nose with a nasal decongestant containing oxymetazoline (Afrin).
Pinch your nose. Use your thumb and index finger to pinch your nostrils shut. Breathe through your mouth. Continue to pinch for 10 to 15 minutes. Pinching sends pressure to the bleeding point on the nasal septum and often stops the flow of blood.
If the bleeding continues after 10 to 15 minutes, repeat holding pressure for another 10 to 15 minutes. Avoid peeking your nose. If the bleeding still continues, seek emergency care.
To prevent re-bleeding, don't pick or blow your nose and don't bend down for several hours. Keep your head higher than the level of your heart. You can also gently apply some petroleum jelly to the inside of your nose using a cotton swab or your finger.If re-bleeding occurs, go through these steps again. Call your doctor if the bleeding continues.When to seek emergency care
- The bleeding lasts for more than 30 minutesYou feel faint or lightheadedThe nosebleed follows an accident, a fall or an injury to your head, including a punch in the face that may have broken your nose
When to contact your doctor
- You experience frequent nosebleeds. You may need to have a blood vessel cauterized. Cautery is a technique in which the blood vessel is burned
with an electric current, silver nitrate or a laser. Your doctor may pack your nose with special gauze or an inflatable latex balloon to put pressure on the blood vessel and stop the bleeding.You're experiencing nasal bleeding and taking blood thinners, such as aspirin or warfarin (Jantoven). Your doctor may advise adjusting your medication dosage.
Apply a water-based lubricant to your nostrils and increase the humidity in your home to help relieve nasal bleeding.
From Mayo Clinic to your inbox
Sign up for không lấy phí, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications any time by clicking on the unsubscribe link in the e-mail.
Dec. 18, 2022
Alter H. Approach to the adult with epistaxis. https://www.uptodate.com/contents/search. Accessed Aug. 1, 2022.Nosebleeds. American Academy of Otolaryngology — Head and Neck Surgery. https://www.enthealth.org/conditions/nosebleeds/. Accessed Dec. 1, 2022..
Nose Bleed Management and Epistaxis
This protocol serves as brief introduction to epistaxis treatment measures, many of which may only be temporizing in nature. For significant or uncontrollable epistaxis, it is recommended that patients immediately be seen by the appropriate emergency response/medical professionals in their area.
see also: Facial Fracture Management Handbook; Epistaxis; Anterior Ethmoidal Artery Ligation; Endoscopic Sinus Surgery; Silver nitrate use and toxicity
EpistaxisNew Latin, from Greek, from epistazein to drip on, to bleed the nose again, from epi- + stazein to drip.
EtiologyTraumatic: digital manipulation, abrasion (post nasal intubation, feeding tube, etc), fractures, etc
Infectious: bacterial
URI
Inflammatory: granulomatous disease, allergic rhinitis
Neoplastic: papilloma (Schneiderian), fibroma (JNA), squamous cell carcinoma, etc
Drug-Induced: aspirin, warfarin, other blood thinners, nasal sprays, chemo/radiation therapy
Systemic: coagulopathy, HTN, thrombocytopenia, DIC, dehydration, liver failure, telangiectatic diseases (see link below)*
Environmental related: dehydration of environment or seasonal air condition, nasal cannula O2, etc.
*KTP laser of intra-nasal telangiectasias (HHT) (with or without Avastin injection)
Some authors tend to classify epistaxis into Local and Systemic causes into which the above etiologies are then grouped.
Pertinent AnatomyAnterior Bleeds: most bleeds tend to involve the region of the anterior nasal septum known as Kiesselbach's plexus or Little's area
Kiesselbach's plexus is formed by the Anterior Ethmoid (from internal carotid > ophthalmic a.), Superior labial (from facial a.), Ascending palatine and Sphenopalatine
arteries (both from maxillary a) .
Posterior bleeds: identification of posterior bleed origin may be hard to perform without proper equipment.
Woodruff's plexus: Confluence of vessels posterior to the middle turbinate that is often involved in posterior bleeds.
Woodruff's plexus is formed from contributions of the sphenopalatine (from maxillary a.), ascending pharyngeal (from external carotid) and the Internal maxillary veins.
Systemic disease and neoplastic disease, as well as many of the causes listed above, may lead to significant alteration of intranasal anatomy. Patients may require significant consideration for treatment beyond the scope of this protocol. However, the emphasis on clinical exam and the determination of the appropriate treatment remain of paramount importance.
Pre-Exam PreparationSECURING THE AIRWAY IS THE FIRST STEP IN TREATMENT
-Whether the patient is in clinic, across the hospital, or across the state, the
first step should be to ensure that they have a stable airway. A pulse-oximeter should be used and attending medical staff should be available to assist as deemed necessary with each case. If the patient has a heart condition then place the patient on a cardiac monitor and make sure there is an IV placed before your arrival. Ask the ER staff to help manage elevated blood pressures.
-Additionally, if the patient is awaiting your arrival, the referring medical staff involved may
have the patient blow their nose and utilize vasconstrictive sprays prior to your arrival.
-This should be preceded and followed by maintenance of digital pressure to the cartilaginous portion of the nose, over the inferior nasal sidewall and the lower lateral cartilage, NOT over the nasal bones more superiorly.
Digital pressure should be held firmly (NO PEEKING or QUICK BREAKS) for least 10 minutes or until arrival of treating physician/ENT. The UIHC ETC has blue clips for
patients to use, which are not as effective as digital pressure, but helpful in elderly patients who cannot maintain pressure for 10 minutes (due to arthitis, etc.)
- Medications
-Vasoconstrictor: Neosynephrine, oxymetazolineProtective wear
-Gown
-Gloves
-Face Mask
-Face Shield/goggles
Each of these protective items should be requested prior to traveling to the ER or procured prior to treatment of patients on the wards or in clinic.
A "quick
look" can turn into a mucous membrane exposure with an abrupt move, a sniff, or a sneeze.
- Supplies
-Head light
-Nasal speculum
-Wall mounted suction system
-Frazier suction tips
-Possible Yankauer suction (for profuse bleeds/OC clearance of blood/clot).
-Possible electrocautery
-1% lidocaine w/ 1:100,000 epinephrine (check allergy status prior to utilization)
-5-10cc syringe
-18 & 27 gauge needles
-Other epistaxis treatment measures shown in more detail below
Some institutions may have an epistaxis tray or room available. The items above are not all necessary for every nosebleed, but should be considered for use in treatment as available.
- Identifying the location of the bleeding is absolutely paramount in epistaxis management. Once appropriate gowning and gloving have taken place, a head light and nasal speculum can often be utilized for initial examination.
-Clot unable to be cleared
by the patient should be suctioned with a large bore frazier suction (as tolerated by patient's anatomy).
-The majority of bleeds will be localized to the anterior septum, often times with an area of excoriation/abrasion or hypervascularity noted.
-Documentation should be noted of the side, size, accessibility of lesion and other physical exam findings, including patient's tolerance of intervention and cooperation.
-If the clot is cleared anteriorly and it appears the bleed is
posterior, a rigid scope and light source should be used, and suction the nose completely to enable visualization of the nasopharynx completely.
-Ideally the bilateral nares will have been sprayed with topical anesthetic and vascoconstrictor once clot is evacuated. Some rapid bleeds may not be conducive to appropriate application. Utilize judgment in waiting for onset of medication versus initiation of treatment.
-Based on exam findings, consider appropriate treatment measures as listed
below.
-Topical vasoconstrictors and digital pressure: May assist with temporizing or stopping some nose bleeds. Inspection for regions of concern and possible further treatment should be made according to presentation, history and clinical status of patient. Sometimes pledgets or a cotton ball soaked in vasoconstrictor and lidocaine can carefully be placed to slow bleeding anteriorly, and in the meantime an injection of ~1 cc of lidocaine 1% with 1:100,000 epinephrine into the greater palatine foramen bilaterally can be helpful in slowing the posterior supply's contribution. Use caution in patients with heart conditions, strongly consider placing on a monitor.
-Cauterization: May be performed chemically (silver nitrate) or with electrocautery. In using either chemical or electrocautery, only one side of the septum should be cauterized to prevent septal perforation, and any cautery. Additionally, only one
side of closely approximating area, such as the middle turbinate or the mid-septum should be cauterized to prevent adhesions. Wait least 2 weeks to cauterize the opposing contralateral side of the septal mucosa if it has recently been cauterized. Suction cautery is very effective but may be contraindicated for patients with a pacemaker/defibrillator or cochlear implant. A pacer/defbillator can be deactivated short term by applying a magnet that is usually found in the ETC (similar
to when in the OR). Call cardiology to get an OK when temporarily turning off someone's pacer/defibrillator, and have ER staff available and IV access established to resuscitate the patient if needed. Bipolar cautery can be safely used but it is difficult to use posteriorly.
- Silver Nitrate: Comes in sticks with silver nitrate the end. Touch stick to area of concern and the surrounding prominent vasculature. Do not blatantly roll over entire septum. Use in directed
manner. Be aware blood and mucous containing silver nitrate can run toward nasopharynx or anteriorly and burn the lip/face or throat. Remove any excess with suction or a plain cotton swab. Cautiously suction excess without further harming friable mucosa. Caution the patient that this intervention will not be pleasant i.e. it will sting/hurt.
-Packing: A variety of packing may be available. If cauterization is unsuccessful, difficult to perform (in posterior bleeds for example), or if the patient is unstable then packing is indicated. The following is not an exhaustive list, but an overview of some of the more popular packs available
-Foley catheter and gelatin-thrombin matrix combination (for posterior epistaxis)
Spray 4% lidocaine/phenylephrine to administer topical anesthesia
Place a 12 Fr Foley catheter into the posterior nasal cavity and inflate with ~5mL of sterile water or saline. This may provide a temporary tamponade. If there is still brisk bleeding seen in the oropharynx, Deflate the foley and pass it into the nasopharynx, inflate it and pull it anteriorly so that it occludes the choana. This will usually redirect the flow of blood anteriorly instead of into the airway.
Prepare gelatin-thrombin matrix product (Floseal or SurgiFlo).
Deflate the foley catheter and move it posteriorly into the nasopharynx so that it occludes the choana. This helps prevent aspiration of blood from a brisk bleed as well as any Floseal/SurgiFlo that is applied.
Attach a 14 Fr angiocatheter to the Floseal/SurgiFlo and pass it along the floor of the nose until until you are as far posterior as you can get.
Apply the gelatin-thrombin matrix to the posterior nasal cavity while continuing to occlude the choana with the foley for 10 minutes.
If bleeding continues, apply second syringe and wait an additional 10 minutes
If there is no further bleeding, irrigate the nose with sterile saline to remove any excess thrombin matrix.
Deflate and remove the foley catheter.
Observe patient for 1 hour- Surgicel
- oxidized cellulose polymer (polyanhydroglucuronic acid). Reported to resorb within 1-2 weeks. May place anteriorly or over abrasions as needed.

Image 1: As seen here, Surgicel comes in sheets that may be folded or cut to size for placement as needed.
- Nasopore
- synthetic, fragmentable, biodegradable foam. May be cut to appropriate size and shape with scissors. Will expand on exposure to fluid. May be inserted with nasal speculum and/or bayonets or with endoscope and bayonets depending on location and clinical scenario.

Image 2: Nasopore in its packaging.

Image 3: Nasopore in its packaging. UIHC Oto utilizes 8cm Extra Firm Nasopore with cutting to size performed on utilization.
- Floseal/SurgiFlo
- Hemostatic matrix (bovine gelatin- human thrombin matrix) that can conform to irregular wound edges. Noted by manufacturer to have proprietary blend of procoagulants including high concentrations of thrombin to react rapidly with the patient's fibrinogen allowing for the formation of a mechanically stable clot. Application
requires a preparation and mixing period, so factor this into the treatment considerations. Once Floseal is applied, a surgical patty should be placed and held over the wound to allow for an appropriate clotting to occur. It is resorbable over 6-8 weeks. Wound should be lightly irrigated so as to remove excess.

Image 4: Floseal in packaging.
Image 5: Floseal prepared in applicable matrix form. Syringe and applicator allow for some mid-posterior nasal application.
Temporary packing: Foley catheter, lamb's wool, strip gauze, merocel, Rhinorocket, Rapid rhino.
These packings must be removed. The duration of packing is variable, but generally from 2-5 days, and should include antibiotic prophylaxis to prevent toxic shock syndrome (Augmentin or 2nd generation cephalosporin) or sinusitis. Absorbable packing does not
warrant antibiotic usage. In general our practice is to pack again if a patient re-bleeds with the first packing removal. If the patient re-bleeds a second time then the next step is generally an OR procedure or IR consult for embolization.
- Foley catheter
- A 12-14F size should be inserted into naris. ~5-10cc of saline should be applied and the filled catheter pulled forward to settle in the choana. A soft bolster should be placed between the nasal
ala/columella and the umbilical clamp that will be placed anteriorly on the catheter to prevent posterior passage of the foley into the naso/oropharynx as well as to prevent columellar necrosis.
- A name brand polyvinyl alcohol sponge that is firm when dry and that
expands as it absorbs liquid. May be cut to size. Original size may allow for easy passage along a relatively straight septum, but once it becomes wet, the expansion that occurs may make it difficult to reposition. Once applied, tape the safety line (pre-attached to the pack) to the cheek to prevent posterior migration and allow for assistance with removal. Prior to removal, soak packing thoroughly. Consider Afrin use pre- and post-removal.
- Medical
grade expandable sponge that comes in a disposable plastic applicator that assists with positioning. Safety string pre-attached to sponge should be taped to cheek to prevent distal migration and to assist with future removal. Prior to removal, soak packing thoroughly. Consider Afrin use pre and post removal.
- Device comes in unilateral 4.5 cm, 5.5 cm (both anterior), 7.5 cm (anterior/posterior) and a bilateral 7.5 cm versions (that are used
UIHC). These devices contain a balloon surrounded by a hydrocolloid (carboxymethylcellulose hydrocolloid (platelet aggregator) coating on inflatable balloon) fabric covering. The balloon allows for a pressurized tamponade of the nasal vessels and the covering theoretically allows for improved ease of insertion and removal as well as hemostasis. Prior to application, device must be soaked with sterile water (H2O, not saline). Balloon may be taped to cheek. Prior to removal, soak packing, deflate
balloon. Consider Afrin use pre- and post-removal.

Image 6: The 4.5 cm, 5.5 cm and 7.5 cm Rapid Rhino devices in their packaging.

Image 7: The packaging and protective wrapper removed, all three devices pre-water soaked with no air added.

Image 8: The devices post-water soak and with air added.
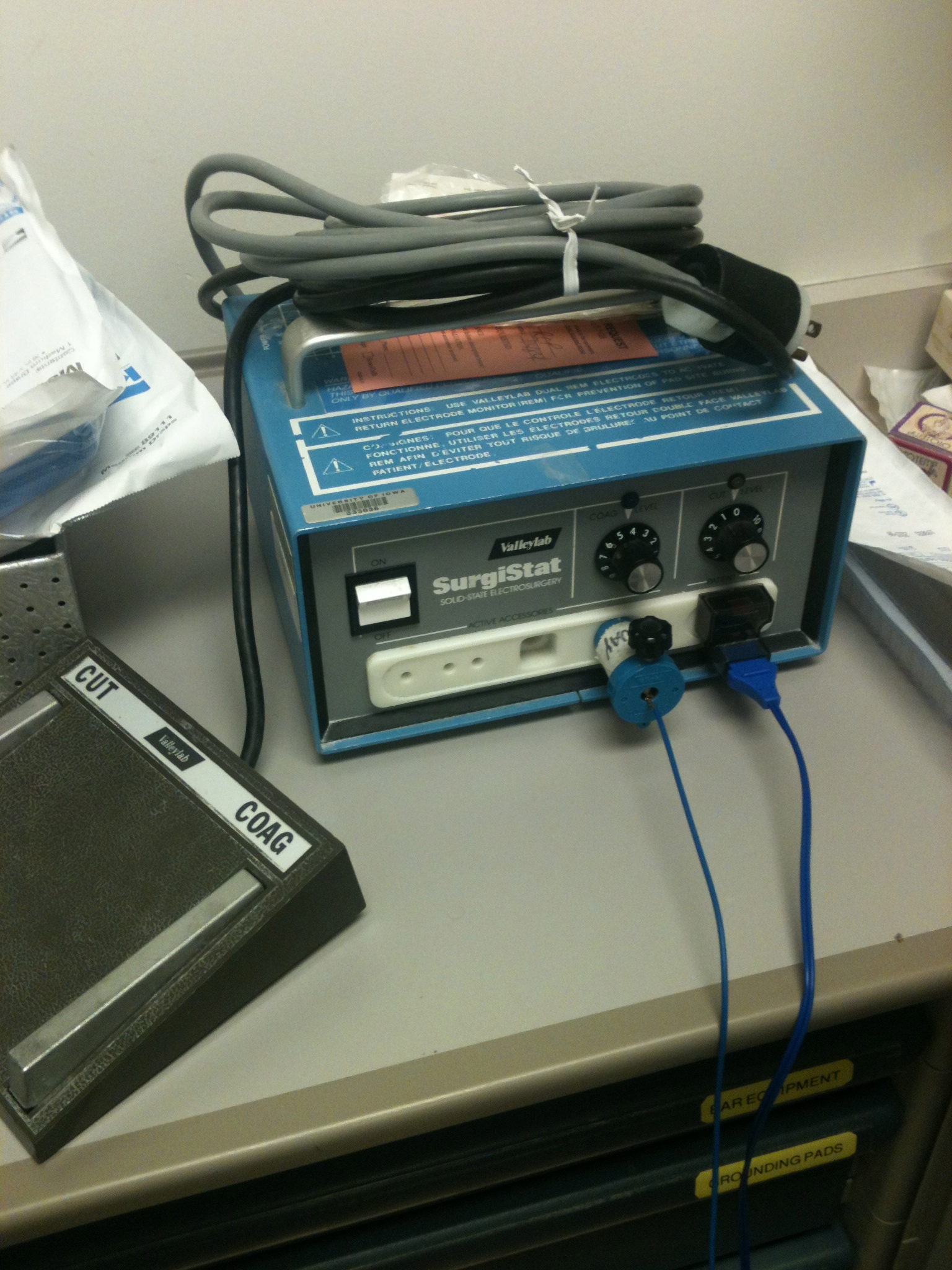
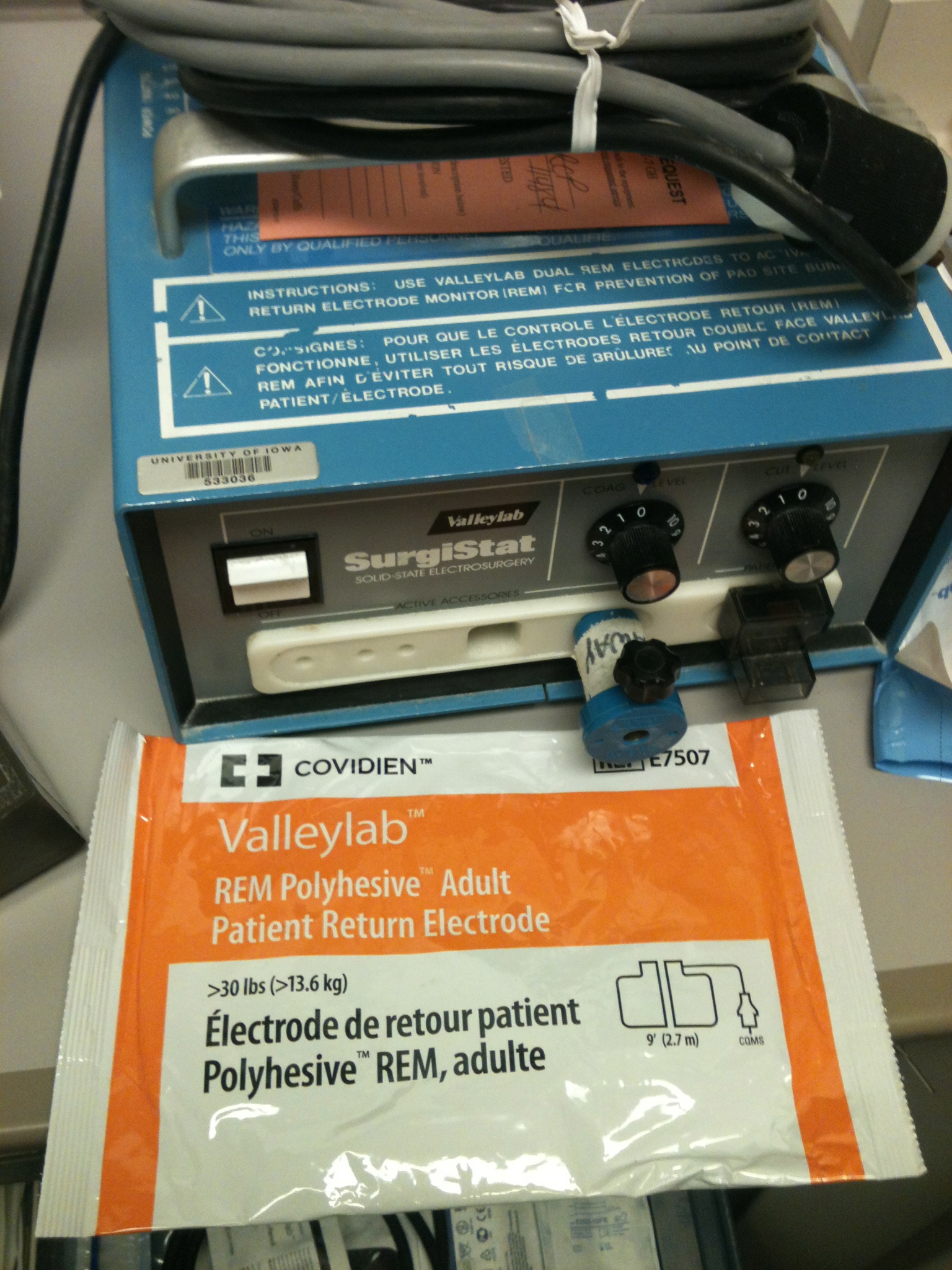
Image 9: Cautery unit in UIHC ER ENT/Ophtho room. Nursing may not be familiar with its setup, so use these images as a guide for setting up suction cautery. Grounding pad inserts on bottom right and monopolar (suction) cautery on left. Note the blue adapter which allows for connection to the monopolar. If this adapter cannot be found someone may have to hold the monopolar wire in contact while you use it.
Surgical InterventionSee also: Anterior Ethmoidal Artery Ligation
- Depending on other injuries, comorbidities and availability of resources, the epistaxis patient may require general intubation. In such
cases, consideration of above measures may still be considered. Additional use of cautery where applicable may be considered. Attempts endoscopic localization and cauterization may be performed in an OR setting if there is a significant bleed or if the patient is proceeding to the OR for other injuries.For severe, persistent or complex bleeds beyond treatment the available measures listed here, consultation of Neuro Interventional Radiology could be considered for
embolization of feeding vessels.
- Avoidance of digital manipulation and trauma.
-Humidified air may assist with moisturizing dry mucous membranes. Use a humidifier home. For inpatients remove nasal cannula and use humidified face mask or face tent.
-Workup of bleeding disorders or systemic diseases by appropriate services if indicated. Correct blood pressure, platelets, uremia, or INR if not
contraindicated.
-Nasal saline sprays and water based gels to anterior vestibule
-Deliver Nasal spray medications with the contralateral hand to contralateral naris technique with avoidance of spraying septum. Consider stopping nasal steroids until episodes abate, as the preparations have alcohol that dry the septum further.
References
Prospective clinical trial of gelatin-thrombin matrix as first line treatment of posterior epistaxis. Kilty SJ, Al-Hajry M, Al-Mutairi D, Bonaparte JP, Duval M, Hwang E, Tse D. - Laryngoscope - ; 124 (1); 38-42Epistaxis: A Contemporary Evidence Based Approach. Barnes, M.L., FRCS-ORL(Ed), MD; Spielmann, P.M., FRCS-ORL(Ed); White, P.S., FRACS, FRCS(Ed), MBChB. Otolaryngologic Clinics of North America, The.September 30, 2012. Volume 45, Issue 5. Pages 1005-1017
Return to [Common Call Problems|protocols:Common Call Problems]
Tải thêm tài liệu liên quan đến nội dung bài viết For a client diagnosed with epistaxis, which intervention would be included in the care plan? Ear disorders Quizlet